Primärtherapie
praetherapeutische Diagnostik
| Obligatorisch | Optional, oft empfohlen | Optional |
| Histologische Diagnosesicherung | ||
| Anamnese | HIV - Test | |
| Körperliche Untersuchung | Feinnadelaspiration der Leisten - Lymphknoten | |
| Rektale Untersuchung | Narkoseuntersuchung | |
| Labor inklusive Nierenwerte | ||
| Proktoskopie | Colonoskopie | |
| Becken- MRI | Transanaler Ultraschall | |
| CT Thorax / Abdomen | PET/CT | |
| Frauen: gynäkologische Untersuchung, CIN /VIN | Geriatrisches Assessment |
Primärtherapie
SCC bis 10 mm
Operation
Radiatio
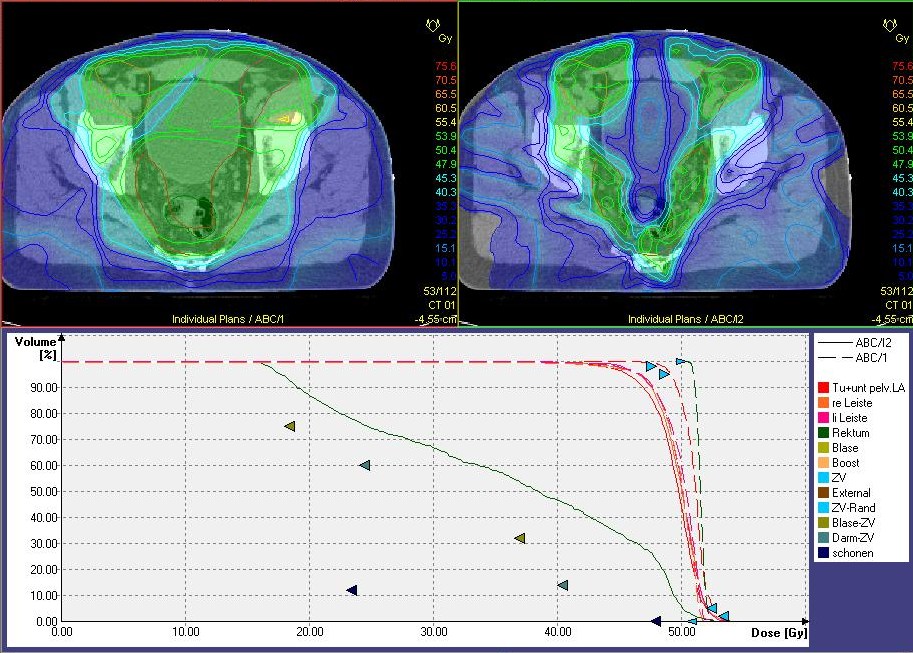
Zielvolumen
Chemotherapie
Epidermoid anal cancer: Results from the ukcccr randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin.
Lancet 1996;348:1049-1054.
2.) Bartelink H, Roelofsen F, Eschwege F, et al.:
Concomitant radiotherapy and chemotherapy is superior to radiotherapy alone in the treatment of locally advanced anal cancer: Results of a phase III randomized trial of the European Organization for Research and Treatment of Cancer Radiotherapy and Gastrointestinal Cooperative Groups.
J Clin Oncol 1997;15:2040-2049.
3.) Flam M, John M, Pajak TF, et al.:
Role of mitomycin in combination with fluorouracil and radiotherapy, and of salvage chemoradiation in the definitive nonsurgical treatment of epidermoid carcinoma of the anal canal: Results of a phase III randomized intergroup study.
J Clin Oncol 1996;14:2527-2539.
4.) Ajani JA, Winter KA, Gunderson LL, et al.:
Fluorouracil, mitomycin, and radiotherapy vs fluorouracil, cisplatin, and radiotherapy for carcinoma of the anal canal: A randomized controlled trial.
JAMA 2008;299:1914-1921.
5.) Glynne-Jones R, et al.:
Anal cancer: ESMO–ESSO–ESTRO clinical practice guidelines for diagnosis, treatment and follow-up.
Radiother Oncol 2014;111:330–339
http://dx.doi.org/10.1016/j.radonc.2014.04.013
6.) Chai CY, Cao HT, Awad S, Massarweh NN:
Management of stage I squamous cell carcinoma of the anal canal.
JAMA Surgery 2018;153:209–15.
doi 10.1001/jamasurg.2017.3151.
7.) Chakrabarti S, Jin Z, Huffman BM, Yadav S, Graham RP, Lam-Himlin DM, et al.:
Local excision for patients with stage I anal canal squamous cell carcinoma can be curative.
J Gastrointest Oncol 2019;10:171–8.
doi 10.21037/jgo.2018.12.12
